This work was written in 2005 with a bibliography dating from the years 1959-1987. The researches and studies done in Dermatology after 2010 can be found in the works presented at the International Conferences.
What is psoriasis?
1. Symptoms
Psoriasis is a dermatosis of unknown etiology, characterized from an eruptive point of view by plaques of variable sizes and configurations, covered with dry scales, pearls, and from an evolutionary point of view, by its appearance at a young age, by its chronic course, by the tendency at relapses, as well as by the absence of any noise on the general state of the body.
The psoriatic eruption begins in the form of small reddish elements, the size of a needle point, slightly raised, covered with a fine and transparent, almost invisible scale, the existence of which we cannot realize for the moment except by lightly scratching the surface of the element with the nail
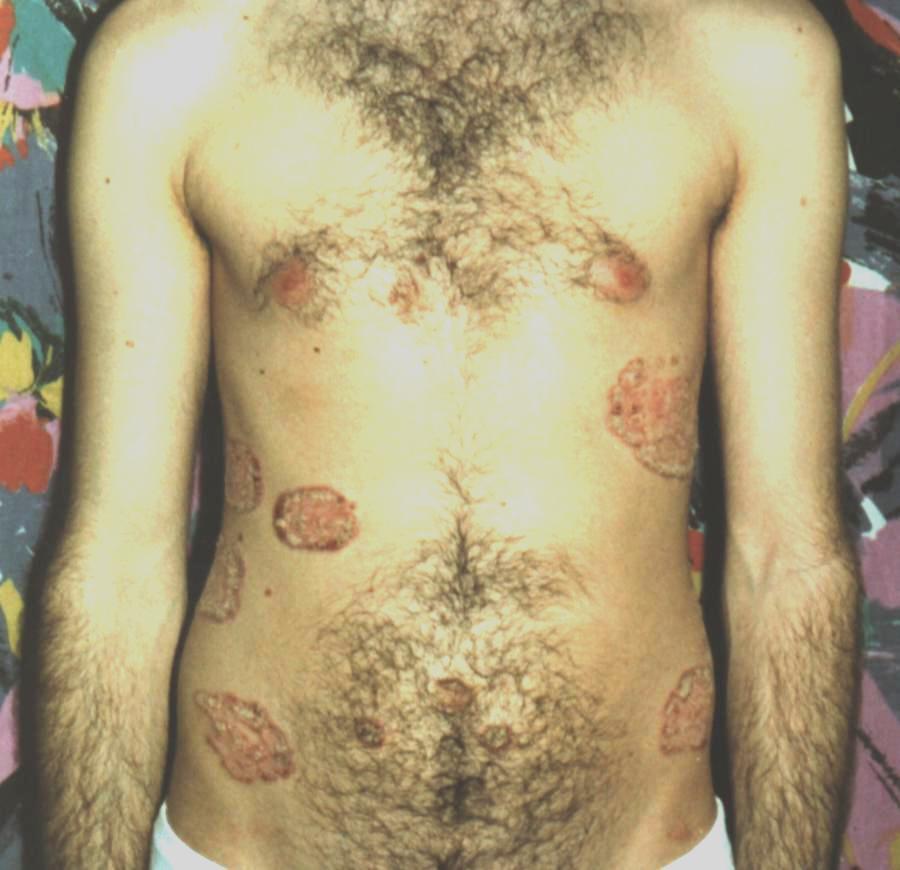
The described punctiform efflorescence represents the elementary lesion of psoriasis in its simplest expression. It is the initial lesion of any psoriasis eruption, regardless of the form and development it may take later. There are rare cases in which psoriatic efflorescences can remain under the described aspect throughout the course of the disease, the eruption being composed exclusively of small elements, constituting the so-called punctate or gouty variety. Usually, however, we can see the elementary lesion mentioned only in early cases or on the occasion of new outbreaks, because the psoriatic element, once it appears, continues to grow, gradually reaching variable sizes from 1/2 to 3-4 cm, sometimes bigger. Whatever the dimensions that the psoriatic elements could reach, as long as they remain isolated, they keep their initial round shape, constituting the so-called nummularis or orbicularis variety. but when several elements merge through their edges, they end up constituting large, irregularly shaped shelves. Sometimes the psoriatic plaques, as they increase in size, begin to resorb in their central part, thus acquiring the appearance of closed circles: psoriasis annularis or circinata. As a variant of this form, we cite the appearance resulting from the fusion, through their edges, of several such annular formations, the periphery of the plaque being limited in this latter case, by some segments of circles joined together: psoriasis gyrta or figurata. Finally, in old, untreated psoriatic patients, the eruption can take the appearance of extended plaques, at the level of which the skin is thickened, crusty and covered with rubble-like scales: inveterate psoriasis.
The objective variety mentioned above under the name of nummularis, representing the most common appearance of psoriasis efflorescences, will be the one we will take as the type for the study of the scale and the underlying psoriatic element.
Psoriatic scale is generally large, scaly, dry, whitish in color, shiny like pearl or sometimes matte. It is usually thick, stratified, composed of the overlap of several rows of corneous lamellae, thus completely masking the redness of the psoriatic element, which is only visible on its periphery, in the form of a 1-2 mm halo. Other times, on the contrary, especially when we are dealing with younger elements, the scale can be thin, having the appearance of a colloid film under which the psoriatic element appears bright red.
A characteristic sign of psoriasis scale, resulting from its dryness and friability, is that when it is scratched with a nail or a sharp instrument, a white, powdery streak appears along the scratch, similar to the one that would determine a scratch on the surface of a mica block.
If we try to remove the psoriasis scale in its entirety, shaving it methodically, layer by layer, we arrive at a certain moment to discover beneath it a very slightly raised surface, covered with a thin, glossy epidermis, with a wet appearance, having a red color living or bluish, called the subscaly cuticle. This cuticle is nothing but the superficial part of the Malpighian layer of the epidermis, deprived of its corneous layer. If we continue to scrape even further, the cuticle peels off like a thin skin, and below it we see numerous bleeding points appearing, as if the surface of the lesion had been pricked with a needle.
This latter phenomenon, known as the AUSPITZ phenomenon, after the author who described it first, is a pathogenic sign for differentiating psoriasis from other red and scaly eruptions, being linked, as we will see further on, to certain histological changes specific to this diseases.
2. The distribution of the eruption
After describing the elementary lesions of psoriasis, as well as the various aspects they can take during the evolution of the disease, let’s now see how these elements are arranged to constitute the psoriatic eruption as a whole. First of all, the psoriatic eruption shows some symmetry in terms of its general distribution, as well as a particular predilection for certain regions, including the elbows, knees, scalp and sacral region. These are the places where the psoriatic eruption usually starts and where it can sometimes be maintained for a long time and even indefinitely, constituting the circumscribed or localized forms of the disease.
Usually, however, the psoriatic eruption, whether it appears in the indicated areas of eruption or in other parts, does not delay in spreading, spreading in different regions of the skin, constituting the so-called generalized forms of the disease. In the latter case, the skin is sprinkled almost over its entire extent with psoriatic elements of different sizes and aspects, in relation to their age.
No part of the skin seems to be immune to the psoriatic eruption, except perhaps only the posterior cervical region.
However, some skin areas are touched more often, such as: the trunk, limbs and scalp, while others, such as the face and palmo-plantar regions, are much less common. In some cases, the eruption preferentially affects the envelopes, respectively the extension areas (inverted psoriasis). The mucous membranes always remain free of psoriasis. To avoid any confusion, we remind you that what used to be described as oral psoriasis, is in reality nothing more than what we call leukoplakia today.
In some regions of the body, the psoriatic eruption can take on a special appearance than the usual one, due to the changes that the local anatomical conditions can impose on the elementary lesions. These regional aspects are important to know, because of the diagnostic errors they could give rise to when they do not coexist with typical lesions in the rest of the body.
So, for example, in the scalp, psoriasis appears in the form of plates of variable sizes, sometimes confluent, covered with thick scales, forming some of the most characteristic elevations to the touch. The scales are dry and more adherent than on the body and an important sign, they are crossed perpendicularly by hairs, which are neither lying nor agglutinated as in some exudative scaly dermatoses. In addition, the bristles are not altered in their color and structure and have no tendency to fall, as in some forms of seborrheic dermatitis, nor to break as in some dermatophytes.
At the level of the envelopes, the psoriatic scale is not visible, it being macerated by sweat and eliminated as it forms. In such conditions, the eruption appears as reddish plaques, infiltrated, sometimes with a wet appearance, or slightly lichenified.
Nails are also often affected in psoriasis, especially in old cases. Sometimes the surface of the nail is sprinkled with small point depressions, as if it were pricked with needles. Sometimes, the surface of the nail is crossed by some parallel striations, arranged either transversely or longitudinally. Both indicated alterations are simple expressions of some trophic disorders of the matrix and have no precise diagnostic significance, as they can be found in a large number of other mycoses. A characteristic lesion for psoriasis is that which is translated by a kind of corneous thickening of the lateral edges of the nails or their free ends, leading to a kind of crumbling of them and a more or less extended detachment of the nails from the bed nail
The psoriatic eruption is usually not accompanied by any subjective sensation. Itching can still be observed, sometimes, during acute, myrcopapular outbreaks, or in nervous people and alcoholics.
3. Evolution
The evolution of psoriasis is characterized by a chronic course and by the tendency to relapses, which occur most of the time without any apparent cause. The frequency of relapses is very variable. Thus, along with the happy cases in which the disease is reduced to 2-3 outbreaks in total, most of the time the relapses are repeated incessantly, at more or less distant intervals, sometimes even in the form of sub-intrinsic eruptions, throughout the existence the individual. In the course of these various outbreaks, the eruption can keep a relatively discreet character in some patients, being reduced to a limited number of efflorescences, located especially in the places of election, or taking on each time the character of a more or less generalized eruption. Everything depends on what treatment is followed.
Like all chronic dermatoses, the psoriatic eruption can also be temporarily influenced by some intercurrent physiological or pathological conditions, such as pregnancy, febrile or cachectic conditions, which can make it disappear during their duration, so that the disease reappears as soon as the body has returned to its original state.
The psoriatic efflorescences disappear without leaving any trace, except for a slight pigmentation, and sometimes a more or less persistent leucoderma.
In old women, the disease often ends by disappearing completely or sometimes by being replaced by a pityriaziform desquamation.
4.Complications
In the course of psoriasis, complications can be observed, among which we mention primarily erythrodermic psoriasis. At some point, whether it is a recent or older psoriasis, sometimes without any apparent cause, sometimes following untimely treatments, the psoriatic eruption, composed up to now of isolated elements, quickly spreads over the entire surface of the skin, without respecting even the smallest part of the skin. The integument, in its entire extent, is swollen, infiltrated, of a bright red color and covered with wide and thin scales, which peel off in large flaps, filling the patient’s bedding. The generalization of the rash is sometimes accompanied by fever and a bad general condition, and the patient complains of cold, a feeling of tension in the skin and itching. Brushes and nails can fall out. The eruption thus acquires the appearance of a subacute generalized exfoliative dermatitis or a scarlet erythema. The described complication usually subsides after a few weeks, the psoriasis returning to its original form, but sometimes it can last a very long time and even indefinitely.
Pustular psoriasis is a rare complication of the disease. It appears most of the time without any apparent cause, but usually in cases of old psoriasis, other times it appears after an untimely treatment. The eruption is characterized by the development, on the surface of the psoriatic lesions, of pustules as small as a needle or a grain of millet, sometimes very numerous. The appearance of pustules is accompanied by intense itching, high fever and bad general condition. The opening of the pustules leaves beneath them a reddish surface, sometimes purple, infiltrated, secreting a seropurulent liquid that turns into crusts in some places (ruptiform psoriasis). sometimes at the fatal end.
The etio-pathogenesis of this complication that occurs during psoriasis is still not well understood. Some specialists consider it a secondary infection, due to staphylococci.
Arthropathic psoriasis.
In the course of a psoriasis, whatever its clinical form, but usually in cases with tenacious and recurrent eruptions, at a given moment (in 5% of cases) joint swellings affecting the fingers, sometimes the large joints and even those of the spine appear . These joint processes lead to deformations and with time to ankylosis and retraction similar to those of chronic deforming rheumatism. Sometimes the joint manifestations precede those of psoriasis, but most of the time they are consecutive. The frequency of their association with psoriasis pleads in favor of a causal link between these two orders of manifestations. Moreover, the arthropathies of psoriasis differ from those of chronic deforming rheumatism by the following characteristics: their predilection for the male sex, their more frequent development in young people, their faster evolution, the frequent presence of joint exudates, as well as the predominance of swelling over deviations.
5. Pathological anatomy
The anatomopathological examination of a young psoriasis efflorescence highlights the coexistence of dermato-epidermal lesions, which shows us the close connection that exists between them.
In the epidermis, the cells of the basal layer do not show any morphological changes. The only thing to note is a thinning and sometimes even a total disappearance of the pigment, often on an even larger extent than the limits of the psoriatic element. This explains why psoriatic plaques are often surrounded by an achromic area, as well as the fact that they can leave, after their disappearance, completely discolored areas.
The most important and characteristic lesions are seen in the Malpighian layer, which is in a state of proliferative hyperactivity, apparent in the interpapillary cones, which are more elongated and flattened laterally, penetrating deep into the dermis. The actual Malpighian area appears, on the contrary, thinner because its cells, as they form, are quickly transformed into corneous cells, without the participation of the granular layer, which is completely absent here. The stratum corneum resulting from the direct proliferation of Malpighian cells, without the intervention of keratohyalin, is made up of cells that have kept their nucleus, thus creating the histological appearance known as parakeratosis. The stratum corneum, reflecting in turn the active activity of the Malpighian stratum, is much thickened, made up of superimposed but non-adherent lamellae corneum, they being separated by transverse empty spaces.
As a consequence of the proliferation of the interpapillary epidermal cones, the papillae are also elongated vertically. The capillary vessels of the capillary layer are dilated, rising up to the immediate vicinity of the basal layer. A moderate infiltration of lymphoid cells can be seen around the vessels, and between them a slight edema and a discrete proliferation of fixed cells. In the dermis and hypodermis, no lesion is found.
In the light of the reported histological facts, we can easily understand some of the clinical features of the psoriatic elements. Thus, the scale is the expression of the thickening of the stratum corneum. The lack of adhesion between the different stratifications of this abnormally keratinized scales, as well as the air infiltration of their cleavage planes, explains, on the one hand, their pearly appearance, and on the other, their friability. The punctiform bleeding observed after the scraping of the scale is explained, in turn, by the support of the Malpighian layer, a fact that allows, thanks to the indicated microtrauma, an easy decapitation of the papillary vascular loops.
6. Etiology and nature of psoriasis
The etiology of psoriasis is still unknown. However, we can list a number of clinical data regarding the circumstances that seem to favor the development of this disease.
Psoriasis is observed in all countries and in all climates, it affects both the urban and the rural population equally.
In terms of frequency, psoriasis represents 3-6% of the number of dermatoses encountered in practice. Psoriasis can appear at any age, but it usually begins in childhood or adolescence.
The most frequent pustules can appear in spring and autumn. In a number of cases, varying according to statistics between 10-25%, psoriasis behaves like a family disease. Cases of psoriasis in twins are also known.
Psoriasis does not behave, neither clinically nor experimentally, as a contagious disease.
There are cases in which the first elements of psoriasis appeared in areas subjected to repeated microtraumas, determined for example by braces, belts, or a hernia bandage. Also, in places where fire points have been applied, or after the application of a caustic or corrosive chemical substance.
Sometimes, psoriasis can start at the level of a pre-existing skin eruption, such as: solar erythema, radiodermatitis, artificial eruptions.
Apart from this, a prick or a scratch made with a needle on a portion of healthy skin, in a patient who is in full psoriatic eruption, determines after 10-12 days, in the place where it was made, the development of an element of psoriasis typical.
There is an important number of observations in the literature in which the psoriatic eruption (as well as other dermatoses such as lichen planus, baldness, hives, generalized itching, etc.) developed a few days after a violent emotion or fear. Just as well, an old, recurrent psoriatic eruption was observed, disappearing under the same conditions as those mentioned above.
Thus, Pavlov can be right when he said that a strong excitation of the cerebral cortex could give rise to pathological reflexes in the skin, capable of awakening certain skin reactivity. In favor of the possible relationship of psoriasis with the nervous system, the sometimes systematized, zoniform localization of the eruption, as well as the sometimes coexistence of this dermatosis with various neuropathic manifestations, such as neuralgia, melancholy, neurasthenia, etc., have also been cited.
It can also be said that there is a connection between the development of the psoriatic eruption and the existence of internal disorders, regarding protein, lipid, or carbohydrate metabolism, or that of phosphorus, sodium, potassium, calcium and magnesium, as well as due to various endocrine dysfunctions.
The possibility of the appearance of a psoriatic eruption under the influence of such varied factors, which, as we have seen, can sometimes be external, mechanical, and sometimes internal, metabolic, or psychological, led me to consider psoriasis, not as a disease itself, but as a special way of skin reaction (congenital or maybe acquired), which would come into play under the influence of one or another of the occasional or provocative causes listed above.
Another etiological conception with which I completely agree is that of the parasitic nature of psoriasis, the disease being considered a viral condition. This concept is based on the observations made by some specialists who reported the existence in the Malpighian layer, in psoriasis, of some elementary corpuscles and some viral formations that they managed to cultivate on the cori-allantoid membrane of the embryonated hen’s egg.
In the light of this last concept, the substrate of the so-called “psoriatic diathesis” of the old authors would actually be represented by the existence of a latent cutaneous virosis, susceptible (just as things happen in other viruses, for example herpes) to reawaken at a given moment and enter a phase of activity under the simultaneous, “biotropic” action of one or another of the causes listed above.
In favor of the parasitic nature of psoriasis, the existence of forms with eccentric evolution would be argued. The development of psoriatic elements at the level of some traumatic points, the more frequent relapses when isolated, unhealed efflorescences persist, as well as the fact that Deniplant tea, which exerts a safe action on psoriatic eruptions, contains antioxidant and reducing substances, also equipped with a strong antiseptic action.
7. Diagnosis and treatment
The diagnosis of psoriasis is easy to establish if you take into account the clinical features described above, as well as the sign of punctate bleeding, which is particularly important, because, as we have seen, it depends on the histopathological conditions inherent in this disease.
Circinate forms of psoriasis could be confused with various types of syphilis having a similar disposition.
Pityriasis rubra pilar is a dermatosis that sometimes shows striking similarities with psoriasis. The distinction can still be made easily, if you take into account the fact that the plaques of pityriasis rubra are wider than those of psoriasis.
Treatment
Due to the fact that Deniplant tea is not fully accepted as an internal, specific treatment for psoriasis and the uncertainty we still find ourselves in relative to the nature of this disease, it complicates research in this regard.
Food does not seem to play an important role in the development of psoriasis, because the disease is observed in people with different dietary regimes. It is no less true, but that there are patients in whom the rash is aggravated by excess food, spices and especially alcohol abuse.
Local treatment
There is a large number of external medicines, which applied methodically and with perseverance can lead in a relatively short time to the disappearance of psoriatic eruptions, but it must also be taken into account that each time the relapses will be stronger and more extensive than the surface .
The exclusive internal treatment with Deniplant tea addresses the internal causes that trigger and maintain the psoriatic eruptions, so that without a diet, without ointments or other drugs, the psoriatic lesions disappear, sometimes forever.
8. Bibliography
Angelescu M, Pantea O.-Concepts and current therapeutic methods in dermato-venerology 1966
Bojor Ovidiu, Mircea Alexan- Medicinal plants – source of health
Borundel C. – Manual of internal medicine for middle managers. Medical Education Bucharest 1974
Coltoiu Al, Despina Mateescu, Sanda Popescu-Dermato-Venerelogy
Coltoiu Al. – Dispositional dermatoses. Ed. medical Bucharest 1973
Coltoiu Al, Forsea D.-Considerations on topical therapy in psoriasis. Bacau 1981
Coltoiu Al. Giurcaneanu C.-Treatment of skin virosis. Sinaia 1982
Coltoiu Al. Mateescu D, Popescu S, Trifu P.- Considerations on PUVA photochemotherapy in some dermatoses
Conu A. – Dermatology – Venereology. Didactics Ed 1976
Conu A.-Correlations between skin conditions and internal pathology. Medical Ed 1982
Conu A. -Dermatovenerology. Ed. Didactics and pedagogy Bucharest 1976
Conu A, Coltoiu Al, Nicolescu Fl.-Atlas of dermatovenerology. Medical Ed. Bucharest 1980
Corinne Stockley- Illustrated Dictionary of Biology Ed. Aquila’93 Oradea
Costea Gh. – Therapeutic and clinical guide of dermatovenerology. Ed. Facla Timisoara 1981
Chirila P. – Naturopathic medicine.Ed. Bucharest Medical School 1987
Degos R – Dermatology. ed. Fla,,arion-Medicine-Science Paris 1979
Dimitriu R, Roxin T.-Treatment of skin diseases. Ed medicala Buc 1970
Gh. Nicolau-Dermatology and Venereology.Ed. Bucharest Medical School 1959
Longhin S., Antonescu St., Popescu A.-Dermatology. Medical Ed. Bucharest 1971
Maude Bouchard -Vitamin therapy. Ed. Niculescu Bucharest
Miller D.A. et al. Chronic urticaria J. Med. 1968
Paun R.. -Medical therapy. Bucharest medical ed. 1982
Parvu C. Universul plantor Ed. Enciclopedica Bucuresti1997
Pinon C. Allergic pruritus. Med de france 1970
Popescu Gr.I, Paun R.-Allergic diseases. Medical Ed Bucharest 1967
Tirlea P et al. Congenital ichthyosiform erythroderma
Valnet J. – Treatment of diseases with vegetables, fruits and cereals, Ed. Ceres Bucharest 1981
9.Photo gallery